“You don’t necessarily have to get on the scales; you see the bones begin to protrude and feel the end is near.” —Patient.
As cancer progresses, significant weight loss emerges as a frequent and distressing symptom in many patients. This weight loss may result from treatment-related side effects, such as difficulty swallowing, nausea, mouth sores, diarrhea, or reduced appetite—all of which heighten the risk of malnutrition. However, weight loss may also result from a syndrome caused by the cancer itself: cachexia, known as wasting syndrome.
Cachexia is a complex syndrome characterized by progressive wasting of skeletal muscle and physical decline. While it is associated with other chronic illnesses, such as chronic obstructive pulmonary disease (COPD), heart failure, kidney disease, and AIDS, it is most commonly observed in cancer patients. Depending on the type of cancer, cachexia affects up to 80% of patients. According to the National Cancer Institute (NCI), it is particularly prevalent in advanced pancreatic and lung cancers, though it also frequently occurs in ovarian, liver, colorectal, and head and neck cancers.
Cancer cachexia not only drastically reduces quality of life but also shortens survival. Patients with advanced cancer and cachexia have significantly poorer prognoses, with the syndrome being the primary cause of death in 20–25% of patients with advanced solid tumors. Therefore, understanding its mechanisms, implications, and treatment strategies is critical to improving outcomes and quality of life.
What is Cachexia?
While there is no universally agreed-upon definition, Cachexia is commonly described as a multifactorial syndrome involving the loss of skeletal muscle (with or without fat loss) that cannot be fully reversed through nutritional support, leading to functional impairment. This condition arises from a negative balance of protein and energy, caused by reduced food intake and abnormal metabolism.
The weight loss seen in cachexia differs from starvation. In starvation, weight loss primarily stems from fat depletion, and the body adapts by producing ketones from fat metabolism to preserve muscle. In cachexia, however, weight loss involves simultaneous depletion of muscle and fat, driven by systemic inflammation and metabolic dysfunction. Unlike starvation, cachexia is resistant to nutritional intervention, highlighting the need for targeted therapies.
Mechanisms of Cancer Cachexia
The development of cancer cachexia involves a complex interplay of metabolic, inflammatory, and neurohormonal factors:
1. Metabolic Imbalance
Cachexia is characterized by an imbalance in energy use, driven by reduced food intake and systemic inflammation. This imbalance leads to energy deficits, increased protein and fat breakdown, and progressive weight loss.
2. Muscle and Fat Breakdown(Proteolysis and Lipolysis)
- Muscle Wasting: Skeletal muscle loss results from decreased protein synthesis and increased protein breakdown via the ubiquitin-proteasome system. Myostatin, proteolysis-inducing factor (PIF), and inflammatory cytokines suppress muscle growth and repair.
- Fat Loss: Heightened lipolysis, driven by tumor-secreted lipid mobilizing factors (LMF), accelerates fat breakdown, contributing to weight loss.
3. Systemic Inflammation
Cancer-induced inflammation triggers widespread tissue damage and metabolic dysfunction:
- Cytokines: Tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), and IL-1β promote muscle wasting, appetite suppression, and increased energy expenditure.
- Immune Cells: Neutrophils, macrophages, and T-cells amplify the inflammatory response, further driving tissue breakdown.
4. Neurohormonal Imbalance
Hormonal disruptions in cachexia impair appetite regulation and muscle maintenance:
- Growth differentiation factors (e.g., GDF-15) and dysregulated leptin and ghrelin(appetite regulating hormones) suppress appetite.
- Insulin resistance and increased energy expenditure worsen muscle and fat loss.
5. Mitochondrial Dysfunction
Impaired mitochondrial function reduces energy production, increases oxidative stress, and contributes to muscle and fat loss. Reactive oxygen species (ROS) exacerbate cellular damage, accelerating the progression of cachexia.
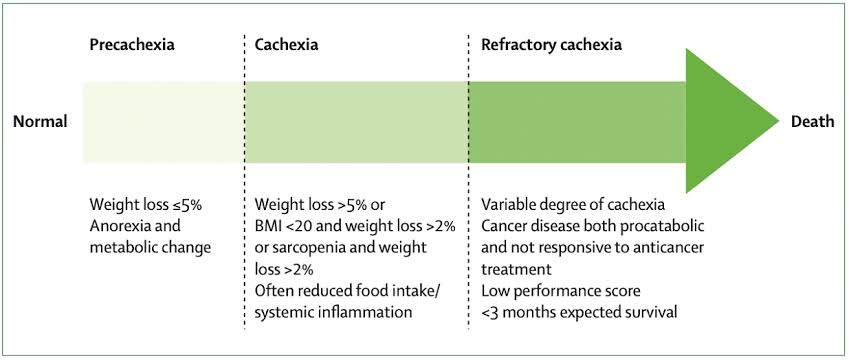
Stages of Cachexia
Cachexia progresses through three clinical stages:
- Pre-cachexia: Early metabolic changes with mild weight loss of 5% or less and anorexia.
- Cachexia: Marked by more than 5% weight loss or body mass index (BMI) below 20 with more than 2% weight loss, or systemic sarcopenia(muscle loss) with weighst loss more than 2%.
- Refractory Cachexia: Occurs when cancer becomes unresponsive to treatment, with a low performance status and survival expectancy of fewer than three months.
Clinical Impact of Cancer Cachexia
Cancer cachexia has widespread effects on the body, and significantly impact patient’s quality of life, underscoring the need for early diagnosis and targeted management to improve patient outcomes. The main clinical impacts include:
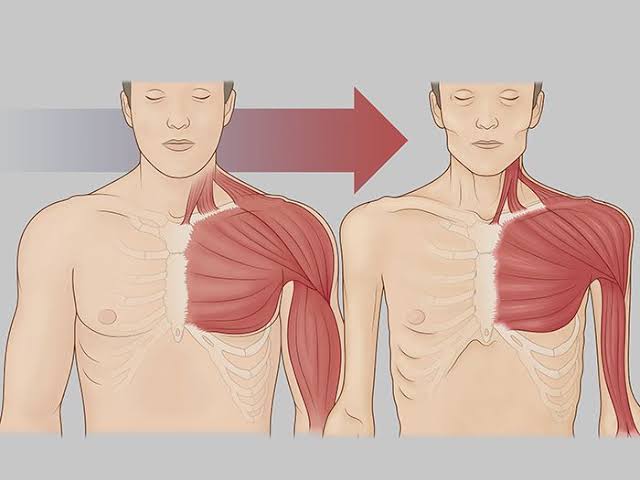
1. Muscle Loss
Muscle wasting is a hallmark of cancer cachexia, and leads to physical weakness, reduced treatment tolerance, and shorter survival. Patients experience increased fatigue, reduced mobility, and a heightened risk of infections and complications.
2. Gastrointestinal Tract Dysfunction
Cachexia alters the gut, pancreas, and liver, leading to nutrient malabsorption and inflammation. Changes in gut microbiota exacerbate systemic inflammation and contribute to muscle and fat loss.
3. Endocrine and Metabolic Dysfunction
Cachexia disrupts glucose metabolism, often causing insulin resistance and reduced energy availability. This differs from typical type-2 diabetes as patients maintain normal fasting glucose levels. Tumor cells consume glucose aggressively, worsening metabolic imbalances.
4. Cardiac Effects
Cachexia weakens heart muscle, leading to fatigue, breathlessness, and reduced cardiac function. Severe muscle wasting can result in heart failure.
5. Bone Health
Cachexia increases the risk of osteoporosis(reduced bone mass) due to muscle loss and changes in bone-regulating proteins like myostatin. Weak bones increase the risk of fractures, falls, and associated complications.
6. Neurological and Psychological Impact
Systemic inflammation affects the brain, disrupting appetite regulation and energy balance. Depression and anxiety are common, compounding the syndrome’s physical effects and further reducing quality of life.
Diagnostic Criteria
The diagnostic criteria for cachexia are defined as the presence of three or more of the following five items:
1) Muscle weakness
2) Fatigue
3) Decreased appetite
4) Low lean body mass, and
5) Abnormal biochemical data (such as, C-reactive protein (CRP), Hb (hemoglobin), and albumin (Alb) levels).
Management Strategies
The management of Cachexia involve both Non-pharmacologic and Pharmacologic approaches:
Non-Pharmacologic Management
1. Exercise
Exercise improves muscle metabolism, insulin sensitivity, and inflammation:
- Aerobic exercise: Enhances energy metabolism and reduces inflammation.
- Resistance training: Strengthens muscles and improves physical performance.
2. Nutritional Support
Nutrition aims to meet energy needs and alleviate malnutrition:
- Tailored dietary counseling and supplementation address nutrient deficiencies.
- Managing nutrition-impact symptoms (e.g., nausea, early satiety) ensures optimal intake.
Pharmacological Interventions
- Appetite Stimulants and weight promoting agents: Olanzapine, Ghrelin analogs (e.g., anamorelin) and megestrol acetate improve appetite and nutritional status.
- Anti-inflammatory Agents: NSAIDs and monoclonal antibodies (e.g.MABp1) target cytokine-driven inflammation.
- Muscle-Preserving and Anabolic Agents: Adrogenic steroids(e.g Nandrolone), Myostatin inhibitors and selective androgen receptor modulators (SARMs) promote muscle growth.
Other Agents
- Cannabinoids (e.g., Dronabinol): Improve appetite but are less effective than traditional stimulants like megestrol.
- Corticosteroids: Temporarily reduce anorexia and fatigue but lack long-term benefits.
- Metoclopramide: Beneficial for patients with delayed gastric emptying or gastroparesis.
Multimodal Therapy for Cancer Cachexia
Multimodal therapy targets the diverse mechanisms contributing to cachexia and provides better outcomes than single-agent treatments.
Examples of Effective Combinations:
- Progestins with Eicosapentanoic acid(fish oil), L-Carnitine, and Thalidomide:Improved appetite, lean body mass, and spontaneous physical activity.
- Beta Blockers and NSAIDs: Helped reduce energy expenditure and weight loss while improving survival.
- Exercise and Nutrition with Pharmacologic Agents:Integration of lifestyle interventions with drug therapy enhances effectiveness and quality of life.
Conclusion
Cancer cachexia is a debilitating syndrome with profound effects on patients’ health and quality of life. Addressing this condition requires a deeper understanding of its pathophysiology, early diagnosis, and the integration of multimodal treatment strategies. Combining exercise, nutritional support, pharmacological therapies, and palliative care can significantly improve outcomes. Advancing research and fostering collaboration between oncologists, dietitians, physiotherapists, and researchers are essential to transforming cachexia into a manageable aspect of cancer care.
Further Readings
Ohnuma T, Ali MA, Adigun R.(2022) Anorexia and Cachexia.
Baker Rogers J, Syed K, Minteer JF.(2023) Cachexia.
Ni J, Zhang L.(2020) Cancer Cachexia: Definition, Staging, and Emerging Treatments.
Mariean CR, Tiucă OM, Mariean A, Cotoi OS.(2023) Cancer Cachexia: New Insights and Future Directions.
Pandey S, Bradley L, Del Fabbro E.(2024) Updates in Cancer Cachexia: Clinical Management and Pharmacologic Interventions. Watanabe H, Oshima T. (2023)The Latest Treatments for Cancer Cachexia: An Overview.
1 Comment
[…] Cancer Cachexia: A wasting syndrome characterized by severe weight loss and muscle atrophy. Read more on Cachexia […]