“When a plant goes to seed, its seeds are carried in all directions, but they can only live and grow if they fall on congenial soil.” — Stephen Paget, 1889
Cancer metastasis remains one of the most formidable challenges in oncology, significantly impacting patient outcomes and treatment strategies.
In his seminal 1889 paper, “The Distribution of Secondary Growths in Cancer of the Breast,” Stephen Paget analyzed 735 cases of breast cancer and observed that metastatic patterns did not merely follow blood circulation, challenging Rudolf Virchow’s earlier suggestion. Paget introduced the “Seed and Soil” hypothesis, likening cancer cells to seeds and specific organs to fertile soil. This idea remains fundamental in explaining why some cancers spread to particular organs. Today, we know that metastasis is a complex, multi-step process involving cancer cells with varying metastatic potentials. Understanding metastasis is crucial for developing effective therapies and improving patient outcomes.
The Metastatic Cascade: A Stepwise Process
Metastasis, the spread of cancer cells to distant organs, is the most lethal aspect of cancer, responsible for the majority of cancer-related deaths. It transforms cancer from a localized disease, potentially curable through surgery or localized therapy, into a systemic condition that is difficult to treat and often incurable. The process of metastasis involves several distinct stages:
- Primary Tumor Growth
Cancer begins at a specific site, forming the primary tumor, such as in the breast, prostate, lung, or liver. Even after the primary cancer has spread to other organs, it is still referred to as the primary cancer of that organ. In other words, prostate cancer that spreads to the bones is still called prostate cancer, not bone cancer.
- Angiogenesis
This is the second stage of metastasis. A tumor cannot grow beyond a millimeter in size unless it attracts new blood vessels. These new blood vessels provide the growing cancer with oxygen and nutrients and create a pathway for cancer cells to spread to other sites in the body.
- Epithelial-Mesenchymal Transition (EMT)
Cancer cells undergo phenotypic changes, becoming more mesenchymal—lacking polarity and gaining motility. This transition enhances their invasiveness, allowing them to migrate from the primary tumor.
- Local Invasion
Cancer cells invade the tissue surrounding the tumor after breaking free from the constraints of their tissue of origin. In normal tissues, cells are held in place by a structured extracellular matrix (ECM), which provides support and prevents migration. Cancer cells invade surrounding tissues by degrading the extracellular matrix (ECM) through enzymes like matrix metalloproteinases (MMPs). They also reduce the expression of adhesion molecules like E-cadherin, loosening cell connections and facilitating spread.
- Intravasation
Once cancer cells invade nearby tissues, they can break through blood vessel walls and enter the bloodstream or the lymphatic system to spread to distant sites. This process of moving through the walls of blood or lymphatic vessels is known as intravasation. Tumor-associated blood vessels are often irregular and leaky, easing this entry.
- Survival in Circulation
Cancer cells in circulation must survive turbulent blood flow and escape detection by immune cells. Imagine a cell going through the heart; it can be likened to a human falling through Niagara Falls. This is why successful metastasis is considered a stochastic event—many cells are killed in circulation by mechanical forces and the immune system.
- Extravasation
When cancer cells reach a target organ, they attach to the blood vessel wall and invade the tissue. This process is called extravasation.
- Dormancy and Secondary Growth
Disseminated tumor cells (DTCs) may remain dormant before proliferating into detectable metastases. During dormancy, disseminated tumor cells (DTCs) do not form detectable macroscopic lesions, and patients show no clinical evidence of disease until relapse months or years later. Studies in early-stage cancers demonstrate that DTCs can be found across multiple organs; however, they eventually grow only in specific tissues in a cancer-specific manner.
Thus, cancer cells must acquire many properties and go through a series of steps to successfully spread to and establish in another organ.
Where Do Cancer Spread?
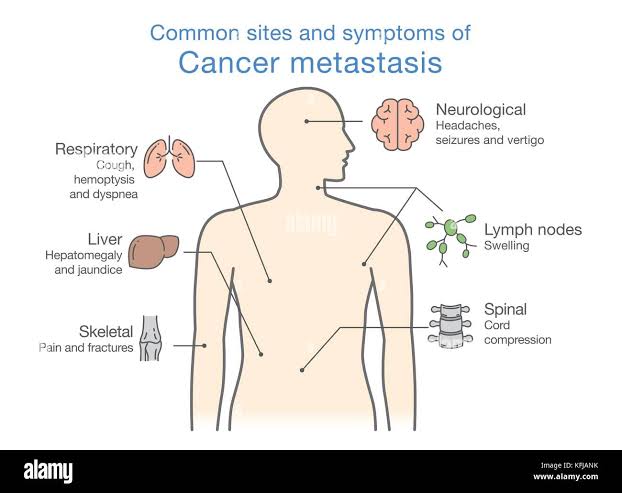
Cancer can spread to almost any part of the body, although different types of cancer are more likely to spread to certain areas than others. The most common sites of metastasis are the bone, liver, lungs, and brain.
The preference of cancer cells for particular organs is influenced by multiple factors, including:
- Circulatory Patterns: Blood flow directs tumor cells to specific organs. For example, the liver, with its dual blood supply, frequently harbors metastases from gastrointestinal cancers.
- Microenvironment Compatibility: Certain tissues provide ideal conditions for tumor survival and growth. Bone metastases, for instance, benefit from the bone marrow’s rich supply of growth factors.
- Immune and Stromal Interactions: The immune landscape and stromal components of target organs can either suppress or facilitate metastasis.
Impact on the Body: How Metastasis Harms and Kills
The spread of cancer to distant organs has devastating consequences for patients. Metastasis disrupts normal organ function, leads to a variety of systemic effects, and complicates treatment. These include:
Organ Dysfunction
Secondary tumors impair vital organ function. For example, liver metastases can disrupt detoxification and protein production, leading to jaundice and body swelling. Lung metastases can cause breathing difficulties, and brain metastases can lead to neurological symptoms and increased intracranial pressure.
Pain and Suffering
Metastatic cancer is often associated with severe pain. Bone metastases are particularly painful, as they erode bone tissue, compress nerves, and increase the risk of fractures. Psychological distress, including anxiety and depression, also significantly affects patients and their families.
Systemic Effects
- Cancer Cachexia: A wasting syndrome characterized by severe weight loss and muscle atrophy. Read more on Cachexia
- Hypercoagulability: An increased risk of blood clots (thrombosis), leading to life-threatening complications such as deep vein thrombosis (DVT) or pulmonary embolism (PE).
- Immunosuppression: Advanced cancer suppresses the immune system, making patients more susceptible to infections.
Therapeutic Implications: Targeting Metastatic Cancer
Treating metastatic cancer remains challenging due to its complexity. Current strategies include:
- Targeting the Metastatic Cascade: Therapies that interfere with specific steps of metastasis, such as MMPs inhibitors, prevent invasion. Anti-angiogenesis drugs like Bevacizumab block vascular endothelial growth factor (VEGF) to limit tumor blood supply.
- Immunotherapy: Immune checkpoint inhibitors like pembrolizumab and nivolumab enhance the immune system’s ability to attack cancer cells,though not all metastatic cancers respond.
- Liquid Biopsies: Detect circulating tumor cells (CTCs) and cell-free DNA (cfDNA) in the blood, aiding real-time monitoring of disease and personalized treatment.
- Combination Therapy: Integrate various treatment modalities, such as chemotherapy, targeted therapy, and immunotherapy, to attack cancer through multiple mechanisms.
- Metastasis prevention: For early-stage cancer patients, preventing metastasis is crucial. Adjuvant therapies like chemotherapy, radiation, or hormonal therapy reduce the risk. Ongoing research aims to identify high-risk patients and develop preventive treatments.
Challenges in Treating Metastatic Cancer
Several factors complicate treatment:
- Heterogeneity: Metastatic tumors can differ genetically from the primary tumor and among themselves, making uniform treatment difficult.
- Drug Resistance: Cancer cells often develop resistance to treatments due to genetic mutations or adaptive responses.
- Access Issues: Some metastases are in locations difficult to reach with surgery or radiation, and barriers like the blood-brain barrier can impede drug delivery.
Future Directions
Advancements in single-cell and spatial technologies are revolutionizing cancer research. Techniques like organoid and mouse models enhance understanding of disease mechanisms and drug responses. Artificial intelligence aids biomarker discovery and drug development, paving the way for innovative treatments.
Conclusion: Conquering Metastasis
Metastasis is the most lethal aspect of cancer, impairing organ function, inducing pain, and leading to systemic effects. While treating metastatic cancer remains,ongoing research into its mechanisms and the development of new therapies offer hope for improved outcomes and prolonged survival. Metastasis is not an inevitable fate. With continued research and innovation, we can disrupt the journey of cancer cells and rewrite the story of cancer treatment and survival.
Further Readings
Gerstberger S, Jiang Q, Ganesh K. Metastasis. (2023)
Fares, J., Fares, M.Y., Khachfe, H.H. et al. Molecular principles of metastasis: a hallmark of cancer revisited. (2020)
Parker AL, Benguigui M, Fornetti J, Goddard E, Lucotti S, Insua-Rodríguez J, Wiegmans AP; Early Career Leadership Council of the Metastasis Research Society. Current challenges in metastasis research and future innovation for clinical translation (2022)
Irani S. Emerging insights into the biology of metastasis: A review article(2019)
Fidler IJ, Kripke ML. The challenge of targeting metastasis(2015)